
Breaking News



Cervical Cancer: How Govt Gambles with Women’s Rights to Reproductive Health

Taking a journey into the lives of some women with cervical cancer, Omolabake Fasogbon in this investigation, reports that it is a not a good time for Nigerian women and girls given that actions and inactions of professionals and government at all levels are fueling the incidence and high death rate from the cancer type
Inside the Gynae B ward of the Lagos State University Teaching Hospital (LASUTH), a reserved section for the low- and middle-class women with all manner of reproductive system cancer, was filled to capacity with patients. While some were newly admitted, some have been on bed for close to three to five months with no significant signs of improvement.
Reflecting high cost of treatment, some, already well and discharged were held down till they are able to settle their medical bills.
With noxious smells wafting through the ward, the whimpering and bawling for early death by the patient, this reporter struggled to hold herself to initiate a discussion with some of the patients, even without a nose cover. Among them was Mrs Gbade (not real name), now deceased, whose ailment was at advanced stage of cervical cancer.
Writhing in pains she struggled to speak to THIDSAY; “I want to die” she cried out severally. As much as she was willing to bare her plight, her strength had failed her. Her husband, who eventually spoke on her behalf, said: “It all started early 2018 with bleeding that is different from her normal menstruation. I took her to Ikorodu General Hospital where after running all tests, it was detected that she had cervical cancer and was referred to LASUTH for proper treatment. But she refused to believe the report, saying, ‘I reject it in Jesus name.
“She refused to go for treatment not until this year that the symptoms became severe. She eventually agreed to visit LASUTH where she ran advanced tests, after which they commenced treatment on her,” Mr Gbade recalled explaining that he has been on and off duty since his wife has been on admission, while his only daughter has stayed away from school just to take care of her mother.
Asides his monthly salary and bank’s savings, he said he has been approaching friends, families, colleagues and micro finance banks to raise over N500,000 for diagnosis and treatment which seemed not to have yielded positive result.
The money he said, also includes N7,500 for meals and bed space paid daily for more than one month. This they did daily before the wife finally died.
Mr Gbade is not pleased with the circumstances leading to his wife’s death despite the amount already spent. He blamed the doctors for not giving her the required treatment.
” I believe the doctors here were responsible for her early demise because two weeks ago, they called to tell me that she was okay and has been discharged but I refused that she should be discharged because all wasn’t well with her. Here is someone declared okay and fit, but could not walk from her bed to the entrance of the ward, still bleeding and yet could not eat. I made sure I bought and did all they asked me to do to avoid excuses. The doctors abandoned her because they said she was at advanced stage.”
Another patient, 55 years old Mrs. Sola, (again not real name) a widow, and nanny is crying for financial support from government and well to do Nigerians to save her life from stage one cervical cancer.
“It all started last year with bleeding, I thought it was my menstruation returning because I had already reached menopause. But when the bleeding became too much and started clotting, I suspected danger which prompted my visit to LASUTH. After series of tests, I was told I have cervical cancer.
“I have been in and out of hospital because I can’t afford to continuously pay for bed space when I’ve not even raised money for all the tests and treatment. My only son is a private school teacher, while I am just a widow feeding on what I get from my nanny job,” she explained.
As the sound of her cry overshadowed her utterances, her 28-year-old son took over the discussion. Trying to hold back tears, he said: “Honestly, I’m tired. This is too much for me. There is no one to turn to and the government is not helping. We were here in July before my mum’s case became this bad, but because we didn’t have money, we were asked to return when we are buoyant. So far, I have spent almost N400,000, yet doctors said they haven’t commenced the proper treatment as she would still need to undergo major surgery”.
Grim Picture
 Gbade and Sola are just a minute number among hundreds of Nigerian women who have either succumbed to cervical cancer or are still battling to get the required treatment. The cancer type is a threat to women folks across the globe and particularly in Africa. Globally, it is recorded that one woman dies of cervical cancer every two minutes.
Gbade and Sola are just a minute number among hundreds of Nigerian women who have either succumbed to cervical cancer or are still battling to get the required treatment. The cancer type is a threat to women folks across the globe and particularly in Africa. Globally, it is recorded that one woman dies of cervical cancer every two minutes.
It is a type of cancer that occurs in the cells of a woman’s cervix — the lower part of the uterus that connects to the vagina. Oncologists explain that it is usually preceded by a curable premalignant stage which can be detected by screening. Like every other cancer type with risk factors, cervical cancer too has its multiple risk factors, notable which is getting infected with human papillomavirus (HPV) usually transmitted via sex, amongst other lifestyle and dietary factors.
WHO records that it is the fourth most frequent cancer in women with an estimated 570,000 new cases in 2018 representing 6.6 per cent of all female cancers. According to the latest statistics published by the International Agency for Research on Cancer (IARC), an estimated 266,000 women die every year from cervical cancer, of which more than 85 per cent live in low-income countries. Without changes in prevention and control, deaths expected to rise to 416,000 by 2035, with over 95 per cent expected to be women living in poor countries like Nigeria.
In 2018, it was reported that about 119,284 new cervical cancer cases were diagnosed while 81,687 women die from the disease in Africa annually.
A recent study from Pan African Cervical Cancer records CC as the most common gynecological cancer . It is confirmed to be the second leading cause of cancer death in women in Nigeria.
In another report by Cervical Cancer Global Crisis Card, Nigeria ranks 5th among countries with regards to death count from CC after India, China, Brazil and Bangladesh .By implication, Nigeria records highest death in Africa.
Cervical Cancer is 70 Per cent Preventable

As deadly as it is, cervical cancer is the mostpreventable cancer type. According to WHO, “Comprehensive cervical cancer control includes: primary prevention (vaccination against HPV), secondary prevention (screening and treatment of pre-cancerous lesions), tertiary prevention (diagnosis and treatment of invasive cervical cancer) and palliative care.”
Scientists have established HPV types (16 and 18) to be primary positive agent for the scourge. It is said that 99 per cent HPV is said to be the positive agent responsible for 70 per cent of cervical cancers and pre-cancerous cervical lesions.
This is why first of all, WHO recommends that two to three doses of HPV immunisation should be given to yet-to-be-sexually-active girls between ages nine to 14 to rule out cervical cancer as they advance into womanhood.
The HPV vaccine is proven nearly 100 per cent effective before a girl child is exposed to sex but less effective in women that are already sexually active.
Founder of Microsoft, Bill Gates,while encouraging countries to invest in HPV vaccine, said, ” CC is one kind of cancer that can be averted of all. HPV is a vaccine now available in basically every rich country and girls have the option of getting the vaccine which is fantastic. This means they don’t get CC .Now in rich countries, you can usually have it and take care of it .But in fact, if you get the HPV infections in a developing country, the chances that it will be stopped is almost zero and so you will get CC as a lot of those women will die. “
However, with 43 per cent of girl children in Nigeria subjected to forced child marriage and accompanying sexual violence, the benefits of the HPV vaccine are more or less nullified by negative cultural practices that undermine the reproductive / sexual health rights of girl children.
Rating the efficiency of screening and treatment of pre-cancerous lesions recommended by WHO, Chief Clinical Oncologists at NSIA-LUTH Cancer Centre, Prof. Francis Durosinmi-Etti (OFR), said, the scourge can be cured if diagnosed at an early stage.
He explained further that while cancer in itself is categorised into four stages, (one to four), cervical cancer advances from zero to five, in which stages three, four and five are the worst of all.
“Cervical cancer can spread to stage three or four within 15 or 30 years depending on the degree of differentiation of cancer cells in the body. This is why regular screening is important to ascertain the health status for immediate treatment before it spreads to aggravation,” he said.
The oncology expert also cautioned against early sex in girls and multiple sexual partners in women, to reduce their risk of contracting HPV infections.
The Founder of Niola Care Foundation, Eniola Saliu Akintunde, advised women to watch their lifestyle and manage to go for regular screening not minding the price. ” HPV infections is limited to sex alone, this is why we have to be cautious of our lifestyle by taking care of ourselves, watch our diet and and even our sanitary pad. We should change our pad at least after 3 hours”
How Government Action Fuels Incidence Rate

As a result of rising incidence of cervical cancer deaths, WHO has declared a global call to action to eliminate CC to reach the goal of elimination through prevention.
In Nigeria however, government efforts to deal with cancer has been more of reactive than preventive.
This accounts for increasing cases and deaths rate,experts have said.
THISDAY investigations revealed that enough is not being done to prevent the debilitating health condition, with treatment access and affordability a herculean task. This situation has given room for investors including government, to allegedly explore and exploit the situation to their gain.
An examination of the various policies and visit to some government hospitals in Lagos confirmed the weak preventive measures being taken across the country.
A case in point is the outcome of Nigeria’s first ‘National Cancer Control Plan’, (NCCP), between 2008-2013. The plan has as its priority: public education, cancer prevention, early diagnosis and referral, effective therapy and palliative care.
While the plan was approved with a budget for implementation, not much was achieved as seen with the absence of HPV vaccine in the national immunisation scheme, high cost of vaccine in few hospitals, poor awareness and enlightenment as well as huge cost of diagnosis.
THISDAY also gathered that the budget for the plan was majorly expended on specious awareness, establishing oncology training for nurses as well as purchase of one accelerator each for Federal hospitals in Lagos, Zaria, Benin and Abuja.
Founder and National Convener, Women Advocates for Vaccine Access, Chizoba Wonodi said, “The awareness on cervical cancer and prevention is quite low. There are no large scale education and information effort from the government around HPV. Several NGOs conduct awareness raising activities, but these efforts are limited and not implemented to cover all states and local governments in the country”.
The recent NCCP was drafted by the former Minister of Health, Isaac Adewole to cover from 2018-2022 . It amongst others give priority to screening services and early detection of cancer,with a promise to make it available for all Nigerians. Also like the first plan, it seeks to attain 90% coverage for Human Papilloma Virus (HPV) vaccine coverage .Looking at the present situation of things in government hospitals, the plan is still dragging.
Although, the Deputy Director and Head, Press and Public Relations, Federal Ministry of Health, Enefaa Bob-Manuel, said, ” the implementation of the policy is going on as planned and all the thematic areas are being implemented concurrently with emphasis on prevention early diagnoses and treatment.”
THISDAY investigations showed that the implementation pace is however slow due to inadequate budgetary provision.
The NSIA- LUTH Cancer advanced Centre is one of the proactive projects undertaken to combat cancer in the country. The project is structured under a public-private partnership (PPP) arrangement between the Nigeria Sovereign Investment Authority (NSIA), and LUTH.
While the establishment of the centre has been commended as it will provide much-needed treatment judging by the level of investment and expertise that went into it, stakeholders believe that more still needs to be done in terms of providing prevention services or have prevention centre in an addition.
For now, the centre is strictly operated as a business venture. The centre is branded as one of the best cancer treatment centre in the world, but it is also one of the most expensive in the country despite being a partnership project with the federal government.
Prohibitive Cost of Treatment and Failure of NHIS
 At LASUTH, despite its inability to handle many of its present cancer cases, it keeps admitting cancer patients who in the end are later referred to other competent hospitals after patients might have spent a lot.
At LASUTH, despite its inability to handle many of its present cancer cases, it keeps admitting cancer patients who in the end are later referred to other competent hospitals after patients might have spent a lot.
In addition to money spent on drugs and other treatments options, patients pay a compulsory fee of N7500 which covers for feeding and bed space for every day they spend in the hospital. Some CC patients stay as long as three to four months in the hospital.
LASUTH does not own a cancer linear accelerator and has only few consultants. It is also still lagging behind in the area of radiotherapy and chemotherapy. “The hospital is still struggling to meet with standards”, our source revealed.
Sharp Practices in LASUTH

A relative of a patient in LASUTH, Mr. Segun (surname withheld), shared with THISDAY how his mother was brought to the hospital and how her situation degenerated before she was referred to UCH in Ibadan.
“A consultant asked me to take my mother to Eko Hospital for radiotherapy because the clinic does not have the facility. This costs about N400,000. Shockingly, when I got to Eko Hospital, I met the same consultant that prescribed the radiotherapy for us in LASUTH, only for the consultant to tell me that my mother does not need the treatment option. This was after I had paid a non-refundable consultation fee of N50,000 and registration fee of N8,000.
THISDAY also learnt of how LASUTH management and doctors collaborate with private laboratories running in the clinic and those operating under PPP structure to generate extra money. These diagnostic centres, despite operating within LASUTH environment, charge as high as laboratories outside.
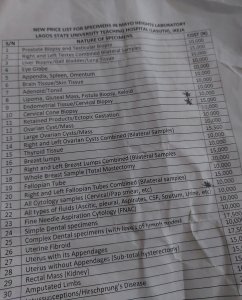
THISDAY also visited some of the private laboratories in LASUTH including BT, Mayo Height as well as state owned laboratory to compare the charges for services. When THISDAY called at the state-owned laboratory to ask for the price of a pap smear, the receptionist directed her to Mayo Height, adding that they don’t run any test that has to do with cancer. Mayo Height collects N10,000 for pap smear and N15,000 for cervical cone biopsy.
In LUTH, pap smear costs N3,500, while cervical biopsy cost N10,600, N600 higher than what MAYO HEIGHT chargers. However, a patient has to be registered with LUTH and bring along his/ her samples before he/ she can be attended to. This means that anyone cannot approach the laboratory for personal screening when not directed by LUTH based doctors
The same tests in Synlab within LUTH compound goes for N10,000 and N14,500 respectively while cervical cone biopsy costs N45,000. When asked if the centre offers HPV vaccine, THISDAY was directed to LUTH.
The Lagos state Health Insurance Plan for which residents pay N45,000 annually does not cover cancer screening, treatment or even HPV vaccine. The state government refused to comment on this when contacted.
One of the reasons responsible for screening lapses and late presentation of cases is the hign price of tests as seen above.
Durosinmi further established this saying , “Women in developing countries often lack access to cervical cancer screening and treatment. About 80 percent of cancer patients present late and advanced stage CC and this is because they do not catch it early”
“This explains why government must come up with accessible screening programmes across all hospitals, at a subsidised rate”, he emphasized.
Although Enefaa Bob-Manuel urged Nigerians to take advantage of the National Health Insurance Scheme (NHIS) for cheap screening service, investigation by our reporter showed that not many of the private laboratories want to identify with the scheme especially with cancer cases.
Government’s Intervention
 But in their defence, the Spokesman for the Federal Ministry of Health (FMOH), Enefaa Bob-Manuel, while explaining how far government has gone in tackling the dreadful disease, disclosed that Nigeria was among the seven benefitting countries of the two and half year’s grant offered through Clinton Access Health Initiative (CHAI) and Unitaid collaboration, to provide cervical cancer screening and possible treatment.
But in their defence, the Spokesman for the Federal Ministry of Health (FMOH), Enefaa Bob-Manuel, while explaining how far government has gone in tackling the dreadful disease, disclosed that Nigeria was among the seven benefitting countries of the two and half year’s grant offered through Clinton Access Health Initiative (CHAI) and Unitaid collaboration, to provide cervical cancer screening and possible treatment.
“Though Lagos, Kaduna and Rivers States are the selected implementing pilot states, government intends to scale up that scheme afterwards. This will further force down the cost of investigating cervical cancer cases,” he said.
By this intervention, one expects that prices of cervical cancer screening should have reduced in the pilot states listed above, but in LUTH, the prices still remain the same.
Implications and Legislation Gaps
 With almost 10,000 lives lost to cervical cancer yearly in Nigeria, this certainly must have impacted negatively on the overall wellbeing of the country.
With almost 10,000 lives lost to cervical cancer yearly in Nigeria, this certainly must have impacted negatively on the overall wellbeing of the country.
The central role of women in society has been proven to ensure the stability, progress and long-term development of nations.
The status of cervical cancer in Nigeria further stresses the need for a legislation on women’s rights to health. The Committee on Economic, Social and Cultural rights,CESCR, and
Committee on the Elimination of Discrimination against Women (CEDAW), state that women’s right to health includes their sexual and reproductive health.
Unfortunately, Nigeria has no specific legislation on women’s right to health and protection from systematic violation of reproductive and sexual health, such as forced child marriage. This is in itself is alarming and most definitely should be addressed by policy makers and all relevant stakeholders.
The growing number of CC case and deaths in the country also points to the need for strengthened legislation and implementation of the Child Rights acts, as well as the fulfillment of Sustainable Development Goal 4 that focused on quality education for both boys and girls.
Statistics shows that there are over 13 million out-of-school children in Nigeria. This factor has been tied to the over 23 million forced child marriage in the country
Forced child marriage has been established to be a factor in girl- child vulnerability to all manners of reproductive and sexual infections, including HPV , the positive agent for CC.
Beyond this, developing countries have been advised to partner with Gavi Alliance to achieve success with primary prevention which is the introduction of HPV vaccine.
This vaccine is a major concern for WHO,who recommends at least 90 percent success rate for countries.
WHO’s Phionah clarified the need for countries to unite with Gavi to introduce the vaccine just like Zambia, Rwanda, Ethiopia and Kenya,amidst other African countries have done.
She said, “while Gavi does not pay 100 percent for HPV vaccine, it was ready to cooperate with any country that shows full commitment. Countries like Zambia, Rwanda, Ethiopia and Kenya,amongst others, have their successes linked to Gavi’s intervention.”
Principal Research Scientist at the Kenya Medical Research Institute (KEMRI), Dr Nelly R. Mugo, also shed some light on how countries can get to introduce the vaccine .
“Government must show full commitment towards the cause. Educating the health care providers and partnership with academia and the media for awareness purpose are also key,” she stated.
On overcoming the cultural misconceptions and superstition around the HPV which is a major challenge to accepting the vaccine in Nigeria, National Coordinator for Cancer Prevention in the Ministry of Health in Zambia, Dr Sharon, Kapambwe, advised on engagement with active stakeholders such as : traditional rulers,community leaders and other influencers to demystify the message to them.
 “This will also ease access to the out of school girls”
“This will also ease access to the out of school girls”
Government has also been enjoined to expand the routine immunisation in the country beyond the current 23 months so as to get the best out of the programme.
Although, Nigerians look forward to effective legislation on Reproductive and Sexual Right, Nigeria already developed a 10-year strategic plan for immunization and primary health care strengthening from 2018 to 2028. HPV introduction is one of the new vaccines to be introduced under this strategic plan.
THISDAY gathered that out of the 3 billion dollars needed to execute this plan, Gavi has already committed to giving Nigeria about one billion dollar based on some principles of engagement and accountability framework.
With Gavi’s commitment, the grant from Clinton Access Health Initiative and the prevention arrangements in the new cancer control plan, stakeholders hoped that Nigeria meant business this time around to tackle the scourge and not the usual promises,procrastination and failures.





